One of the most commonly asked questions at a breast reduction consultation is also one of the hardest to answer precisely: what cup size will I end up? It seems like it should be straightforward — you go in as an F, you come out as a C. But the reality of breast reduction surgery is considerably more nuanced than that, and understanding why will help you approach your consultation with realistic expectations and the right questions.
At Centre for Surgery in London, our surgeons perform breast reduction surgery on patients across a wide range of starting sizes and with a wide range of goals. Some patients want the smallest possible result; others want a meaningful reduction but wish to retain some fullness. Most want to feel proportionate, comfortable, and free from the physical symptoms that drove them to seek surgery in the first place. What they all have in common is that they want to know what they will look like afterwards — and it is the job of a good breast reduction surgeon to help them understand both what is achievable and what influences the final outcome.
Why Bra Size Is Not a Precise Surgical Target
The first thing to understand is that bra cup size is not a standardised measurement. A C cup from one manufacturer is not the same as a C cup from another. Cup size is expressed as a relationship between your band measurement and your bust measurement — the same cup letter means different things at different band sizes. A 32C and a 38C have very different volumes of breast tissue; the letter alone tells you very little about the actual amount of tissue present.
This matters because surgeons do not remove “two cup sizes” of tissue. They remove a specific weight and volume of breast tissue — measured in grams — based on clinical assessment of your anatomy, your symptoms, and your stated goals. The resulting cup size depends on how your remaining breast tissue sits on your chest wall after the procedure, how your bra fits relative to the new shape, and which brand or style of bra you choose to wear afterwards. Two patients who have exactly the same amount of tissue removed may end up wearing different cup sizes simply because their chest width, breast shape, and personal bra preferences differ.
This is not a limitation of surgery — it is simply the reality of how bra sizing works. It is why experienced surgeons describe the target outcome in terms of proportionality and physical symptoms rather than a specific letter, and why patients who fixate on a particular cup size as the primary goal of surgery sometimes find the experience less satisfying than those who focus on shape, comfort, and overall proportion.
What Surgeons Actually Plan for
When your surgeon assesses you for breast reduction, what they are actually planning is the removal of a specific amount of tissue from each breast, guided by several clinical criteria.
Your Starting Volume and Anatomy
The surgeon assesses the current volume of each breast, the degree of ptosis (drooping), the skin envelope, the position of the nipple-areola complex, and the width and projection of the breast. These measurements inform how much tissue can safely be removed while achieving a good shape, maintaining nipple viability, and producing a result that will hold well over time.
Your Symptoms and Physical Goals
For many women, the primary motivation for breast reduction surgery is physical — chronic back, neck, and shoulder pain, bra strap grooving, skin irritation beneath the breast fold, and difficulty exercising. As explored in our post on large heavy breasts and back pain, the weight of breast tissue has a direct and measurable impact on the musculoskeletal system. Where physical symptoms are the primary driver, your surgeon may recommend a more substantial reduction than you might have initially considered, because the symptom relief tends to be proportional to the amount of tissue removed.
Proportionality to Your Frame
A good breast reduction result looks natural and proportionate to the patient’s overall body size and shape. A petite woman with a narrow frame will typically look best with a smaller result than a taller woman with a broader chest — even if both patients describe their goal as “a C cup.” This is why your surgeon assesses your full frame, not just your breast measurements, when planning the procedure.
The Minimum Threshold for NHS Funding
For patients who qualify for NHS-funded breast reduction, there is typically a minimum amount of tissue that must be removed per breast — usually 500g per side — for the procedure to meet the clinical threshold for funding. If you are pursuing surgery privately, there is no such minimum, and your surgeon can tailor the amount removed to your individual goals. Our post on breast reduction for dense breasts covers some of the specific anatomical considerations that affect planning.
How Much Is Typically Removed — and What Does That Mean in Cup Sizes?
As a rough guide — and it is genuinely rough — each cup size difference corresponds to approximately 150–200cc of breast volume, though this varies significantly between individuals. Removing 300–400g of tissue per breast might reduce a patient from an F to a D cup, or from a G to an E cup, depending on their anatomy. Removing 600–800g per side — a more substantial reduction — might take a patient from an H to a D, or from a G to a C.
These are approximations rather than predictions. The volume removed in grams (the weight of excised tissue) does not translate directly to cup size change because of the variables discussed above. What your surgeon can tell you with much greater confidence is how much tissue they plan to remove, what the expected shape and projection of the result will be, and whether the outcome is likely to bring you into a range where standard bras are comfortable and readily available — which is, for many patients, a more meaningful goal than a specific letter.
The “D Cup Goal” — Is It Realistic?
Many patients come to consultation with a specific target in mind, most commonly a D cup or a C cup. For some patients, this is entirely achievable; for others, it may be too small a reduction relative to their frame, creating a result that looks undersized and out of proportion. For others still, particularly those with very large breasts or significant ptosis, aiming for a C cup would require removing so much tissue that nipple viability could be compromised — a clinical risk that no surgeon should take for an aesthetic target.
Your surgeon will discuss what is realistically achievable for your anatomy. If your stated goal is a C cup and the surgeon tells you a D or E is the right result for your frame, this is not a limitation — it is experienced clinical judgement aimed at ensuring the best possible outcome for your specific body.
The Role of Incision Technique
The technique used for breast reduction affects not only the scar pattern but also the shape, projection, and upper pole fullness of the final result — all of which influence how the outcome looks and how bras fit afterwards.
The Anchor (Wise Pattern) Technique
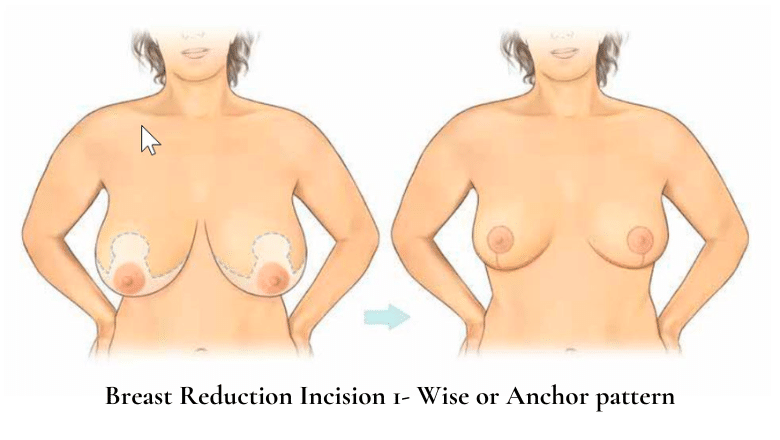
The anchor technique — also called the Wise pattern or inverted T — involves three incisions: around the areola, vertically from the areola to the breast crease, and horizontally along the inframammary fold. This technique allows for the greatest amount of tissue removal and the most control over shape, making it the preferred approach for larger reductions and patients with significant ptosis. Our dedicated post on anchor incision breast reduction explains this technique in detail.
The Lollipop (Vertical Scar) Technique
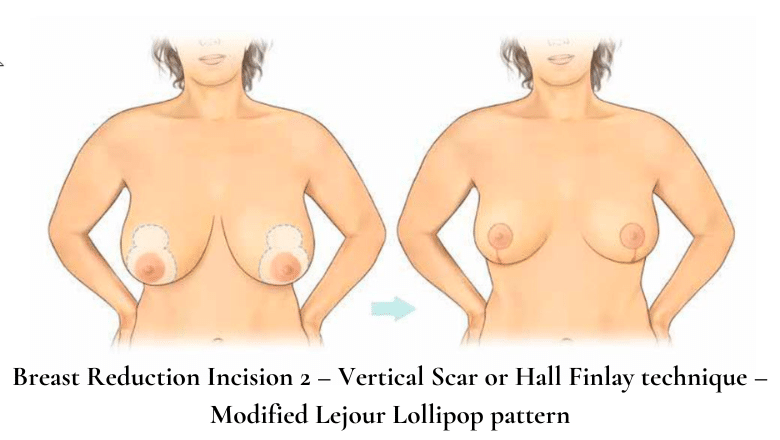
The lollipop technique — also called the vertical scar or Hall-Findlay technique — uses two incisions: around the areola and vertically from the areola to the breast crease, without the horizontal component. This produces less scarring than the anchor technique and is well suited to moderate reductions where the degree of ptosis is not too severe. The differences between these approaches are covered in detail in our post on anchor vs lollipop breast reduction.
Liposuction-Only Reduction
For selected patients — typically those with fatty rather than glandular breast tissue and minimal ptosis — a liposuction-only breast reduction can achieve a meaningful reduction in volume without any significant scars. This technique is limited in how much tissue it can remove and does not address ptosis, but for the right patient it offers a less invasive route to a smaller size.
What Happens to Nipple Position After Reduction?
One aspect of breast reduction that directly affects the final appearance — and the way bras fit — is the repositioning of the nipple-areola complex. In most breast reduction techniques, the nipple is lifted to a higher position on the breast mound as part of the procedure. The areola is typically also reduced in size to remain proportionate to the smaller breast. The implications for nipple sensation and future breastfeeding are covered in our dedicated post on nipple sensation after breast reduction.
Can You Combine Breast Reduction with a Lift?
In many cases, breast reduction surgery incorporates lifting as an inherent part of the procedure — reducing volume and repositioning the nipple naturally elevates the breast profile. The distinction between a breast reduction and a breast lift and when each is more appropriate is an important one to discuss at consultation.
What to Expect at Your Consultation
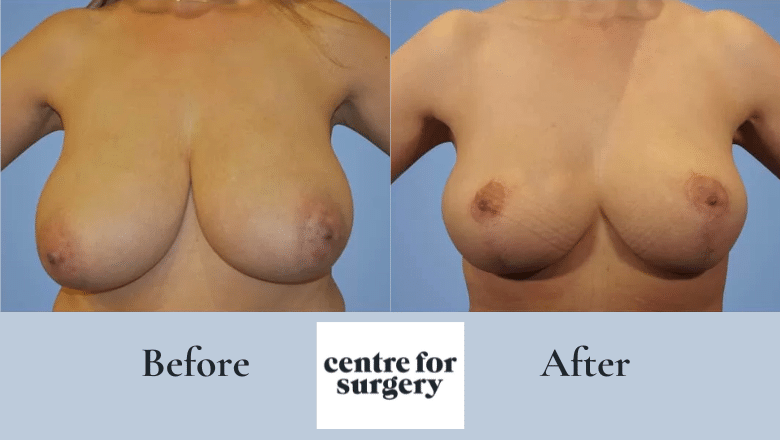
The consultation for breast reduction at Centre for Surgery is a detailed, unhurried assessment. Your surgeon will take a full medical history, examine your breasts, and take measurements. They will discuss your physical symptoms, your aesthetic goals, and your expectations in depth. Before and after photographs of previous patients with similar anatomy are typically shown so you can see realistic examples of achievable outcomes.
The most productive consultations are those where patients come prepared to discuss their goals in concrete, descriptive terms rather than in cup sizes alone. Phrases like “I want to be able to exercise comfortably without a specific sports bra,” “I want my breasts to look proportionate to my frame,” or “I want to be free of shoulder grooving and back pain” give your surgeon far more useful information than “I want to be a C cup.”
If you have concerns about risks — including those covered in our post on breast reduction risks — raise them at this stage. There is a mandatory two-week cooling-off period between your consultation and surgery at Centre for Surgery.
What Changes After Surgery — and What Stays the Same
After breast reduction surgery, swelling takes several weeks to resolve fully. Most patients see the early result at six to eight weeks, but the final shape is not fully visible until around six to twelve months post-surgery. Significant weight gain can cause the breasts to enlarge again. Pregnancy changes the breast irrespective of previous surgery, and breastfeeding may or may not be possible depending on the technique used. Our post on whether you can have a second breast reduction covers what happens if breasts enlarge again in later years.
Frequently Asked Questions
Can my surgeon guarantee what cup size I’ll be after breast reduction?
No — and be cautious of any surgeon who claims they can. Bra cup sizes are not standardised, and the final result depends on your anatomy, how you heal, and what bras you choose to wear afterwards. Your surgeon can tell you how much tissue they plan to remove and describe the expected shape and proportionality of the result, but a specific cup letter cannot be guaranteed.
What is the minimum amount of tissue removed in breast reduction?
There is no universal minimum for private surgery — the amount removed is tailored to your goals and anatomy. For NHS-funded procedures, most trusts require a minimum of 500g per breast. At Centre for Surgery, the amount removed is planned individually for each patient.
Will my breasts be symmetrical after reduction?
Achieving excellent symmetry is a primary goal of every breast reduction, and in most cases the result is a marked improvement on pre-operative asymmetry. Perfect symmetry is not guaranteed — natural breasts are rarely identical — but your surgeon will work to achieve the most balanced outcome possible.
How soon can I go bra shopping after breast reduction?
Most surgeons recommend wearing a supportive post-surgical bra for the first six weeks following surgery. Many patients find it worthwhile to wait until around three to six months post-surgery before investing in a full new bra wardrobe. Tips for supporting the breasts during recovery are covered in our dedicated post.
Is breast reduction available on the NHS?
In some cases, yes — if the procedure meets the clinical threshold for your local NHS trust, typically based on the amount of tissue to be removed and the presence of documented physical symptoms. Many women who qualify clinically are denied NHS funding due to local commissioning policies, and choose to have the procedure privately.
Can I have a breast reduction if I plan to have children?
Yes, though many surgeons recommend waiting until your family is complete if possible, as pregnancy can cause the breasts to change in volume and shape after surgery. This is an important discussion to have at your consultation.
Breast Reduction at Centre for Surgery
Centre for Surgery performs breast reduction surgery at our CQC-regulated Baker Street clinic in central London. Our GMC-registered consultant plastic surgeons bring extensive experience to every procedure, taking a thorough, anatomy-first approach to planning that prioritises proportionality, physical comfort, and a natural-looking result.
All consultations are with your operating surgeon — there is no patient coordinator standing between you and the person who will perform your surgery. Finance options including 0% APR are available through our partner Chrysalis Finance — visit our Finance Options page for details.
Phone: 0207 993 4849 | Email: contact@centreforsurgery.com | Address: 95-97 Baker Street, London W1U 6RN
Learn More
- BAAPS — Breast Reduction Patient Information
- BAPRAS — Guide to Breast Reduction
- NHS — Breast Reduction Surgery

[contact-form-7 id=”256″ title=”Treatments form”]