A soft lump beneath the skin is one of the most common reasons patients present to a plastic surgeon’s clinic. The two most frequently encountered causes are lipomas and cysts — and while both are entirely benign, they are distinct conditions with different origins, different characteristics, and different treatment approaches. Understanding the difference between the two is useful both for patients who have noticed a lump and want to know what they are dealing with, and for those who have been told they have one or the other and want to understand what that means in practice.
At Centre for Surgery in London, our surgeons assess and remove both lipomas and cysts regularly at our Baker Street clinic. In this guide, we explain what each condition is, how to tell them apart, and what the treatment options are for each.
What Is a Lipoma?
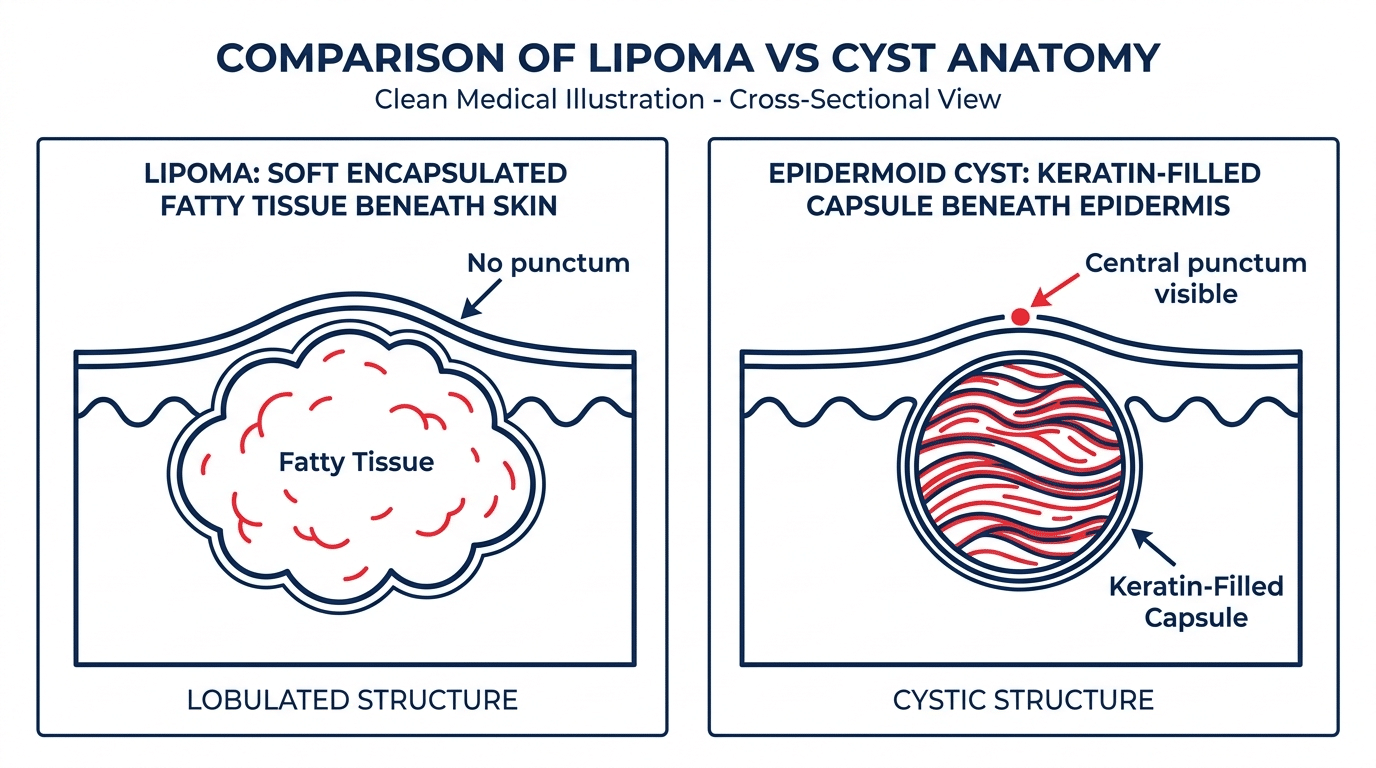
A lipoma is a benign, slow-growing tumour composed of mature fat cells. It develops within the subcutaneous layer — the layer of fat that lies beneath the dermis — and is enclosed within a thin fibrous capsule that separates it from the surrounding fatty tissue. Lipomas are the most common soft tissue tumour in adults, with an estimated prevalence of approximately one in every hundred people. They can develop virtually anywhere on the body where subcutaneous fat is present, though they are most common on the upper back, shoulders, neck, upper arms, and thighs.
A lipoma feels distinctly soft — often described as doughy or rubbery — and moves freely beneath the skin when pressed. It is non-tender in the vast majority of cases, though lipomas overlying a nerve can occasionally cause discomfort. They grow slowly, typically over months to years, and rarely exceed five centimetres in diameter, though larger lipomas do occur. Most lipomas are solitary, but some patients develop multiple lipomas — a condition known as lipomatosis, which in some cases has a hereditary component.
The precise cause of lipoma formation is not fully understood. A genetic predisposition is present in some cases, and there is evidence that minor trauma to fatty tissue can occasionally trigger lipoma development. They are more common in middle age and show a slight male predominance. They are not caused by diet, lifestyle, or weight — lipomas occur in people of all body types, including those with very little subcutaneous fat.
Lipomas are benign and do not become malignant. Lipoma removal at Centre for Surgery includes sending all excised tissue for histological analysis as standard — providing patients with a confirmed benign diagnosis following their procedure.
What Is a Cyst?
A cyst is a sac-like structure with a defined wall that contains fluid, semi-solid material, or gas. In the context of skin lumps, the term usually refers to an epidermoid cyst — the most common type of benign skin cyst in adults. Epidermoid cysts form when epidermal cells become trapped beneath the skin surface, usually at a blocked hair follicle or a site of minor skin trauma. The trapped cells continue to produce keratin, which accumulates within the cyst wall, forming the thick, pale, cheesy material characteristic of epidermoid cysts.
The term sebaceous cyst is widely used but technically imprecise — true sebaceous cysts are considerably rarer and arise from the sebaceous glands themselves, rather than from trapped epidermal cells. In everyday clinical practice, when a GP or patient refers to a sebaceous cyst, they are almost always describing what is technically an epidermoid cyst. For a detailed explanation of this distinction, see our guide to sebaceous cyst vs epidermoid cyst.
Epidermoid cysts are most common on the face, neck, scalp, back, and chest. They present as smooth, round, mobile swellings beneath the skin, and a characteristic central punctum — a small dark opening on the skin surface — is often visible. Cysts are generally non-tender unless inflamed or infected, at which point they can become rapidly painful, red, hot, and swollen. Cyst removal at Centre for Surgery involves complete excision of the cyst capsule — the only way to reliably prevent recurrence.
Lipoma vs Cyst — The Key Differences
While both lipomas and cysts present as smooth, mobile lumps beneath the skin, several clinical features allow them to be distinguished from each other in most cases without the need for imaging.
Feel and Consistency
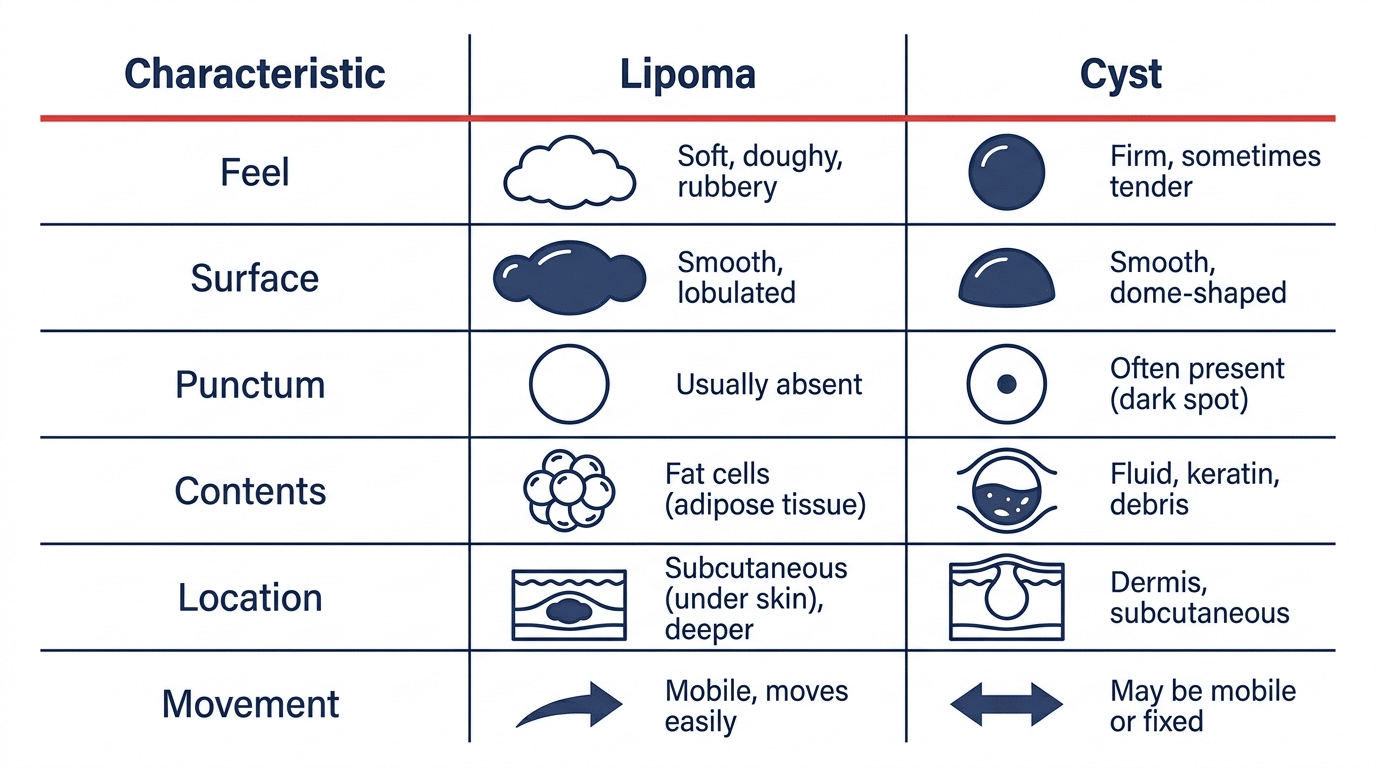
This is often the most immediately distinguishing feature. A lipoma feels soft, doughy, and compressible — it yields easily to pressure and feels as though it is composed of loosely packed material. A cyst, by contrast, feels firmer and more tense — it has a defined, spherical quality and feels as though it contains pressurised material. Experienced clinicians often describe the feel of a cyst as similar to a grape or a marble beneath the skin.
Presence of a Punctum
One of the most reliable distinguishing features of an epidermoid cyst is the presence of a central punctum — a small, dark opening on the skin surface that marks the blocked follicular opening through which the cyst formed. Lipomas have no punctum — the overlying skin appears entirely normal, with no visible surface feature. If you can see a small dark spot on the surface of a lump, it is almost certainly a cyst rather than a lipoma.
Depth
Lipomas sit in the subcutaneous fat layer, which means they lie somewhat deeper beneath the skin surface than epidermoid cysts. Epidermoid cysts develop just beneath the dermis and therefore sit closer to the surface, giving the overlying skin a more tented or stretched appearance in some cases.
Mobility
Both lipomas and cysts are mobile beneath the skin, but they move differently. A lipoma tends to slip away from the examining finger — it glides freely through the surrounding fat. A cyst tends to move with the overlying skin — because the cyst wall is attached to the dermis at the punctum, pressing the cyst causes the skin above it to move with it.
Contents
A lipoma contains mature fat cells — soft, yellowish, lobulated tissue that is visible on opening the specimen at surgery. A cyst contains keratin — a thick, pale, cheesy material with a characteristic odour. These are entirely different substances, and the difference is immediately apparent during surgical removal.
Inflammation and Infection
Lipomas very rarely become inflamed or infected. Cysts, by contrast, have a well-recognised tendency to become inflamed — the cyst wall can break down spontaneously or following minor trauma, causing the keratin contents to provoke a strong inflammatory response in the surrounding tissue. If a lump that has previously been soft and asymptomatic has suddenly become red, hot, swollen, and tender, this is almost always a cyst that has become inflamed rather than a lipoma. As covered in our guide to cyst recurrence, an inflamed cyst requires treatment of the acute episode before surgical removal can be planned.
Location Patterns
While both can occur almost anywhere on the body, lipomas are more common on the trunk, upper arms, and thighs. Cysts are particularly common on the face, neck, scalp, and back. A lump on the scalp is considerably more likely to be a pilar cyst than a lipoma.
Can You Tell the Difference at Home?
In many cases, the clinical features described above make it possible to form a reasonable impression of which type of lump you have. A soft, painless, slowly growing lump on the upper back or shoulder with normal overlying skin is very likely a lipoma. A firm, spherical lump on the face or neck with a small dark spot on the surface is very likely a cyst. However, self-examination has significant limitations — the feel of a lump, its depth, and its relationship to the overlying skin are all better assessed by an experienced clinician than by a patient examining their own body.
There are also several other conditions that can present as subcutaneous lumps and that require professional assessment to distinguish — including lymph nodes, ganglion cysts, fibromas, vascular lesions, and in rare cases more serious pathology. Any new lump, any lump that is growing, any lump that is hard rather than soft, any lump that is fixed rather than mobile, or any lump accompanied by systemic symptoms should be assessed by a doctor promptly rather than self-diagnosed. Choosing a specialist clinic for lumps and bumps assessment ensures that a thorough clinical examination is performed and any uncertainty is appropriately investigated.
Do Lipomas and Cysts Need to Be Removed?
Neither lipomas nor cysts require removal for medical reasons in most cases — both are benign and neither poses a health risk. The decision to remove is based on the patient’s individual circumstances, symptoms, and preferences.
Common reasons patients choose to have a lipoma removed include: the lipoma is in a prominent or visible location and causes cosmetic concern; it is growing and becoming larger over time; it is in a location where it causes discomfort from pressure on surrounding structures; or the patient wants histological confirmation of the benign diagnosis.
Common reasons patients choose to have a cyst removed include: it has previously become inflamed; it is in a visible location causing cosmetic concern; it is growing; or it is in an awkward location that causes practical difficulty. Patients who have experienced a cyst infection are strongly advised to arrange elective removal during a quiescent period — removing a calm, non-inflamed cyst is a considerably cleaner and more straightforward procedure than managing an acutely inflamed one.
How Are Lipomas and Cysts Removed?
Lipoma Removal
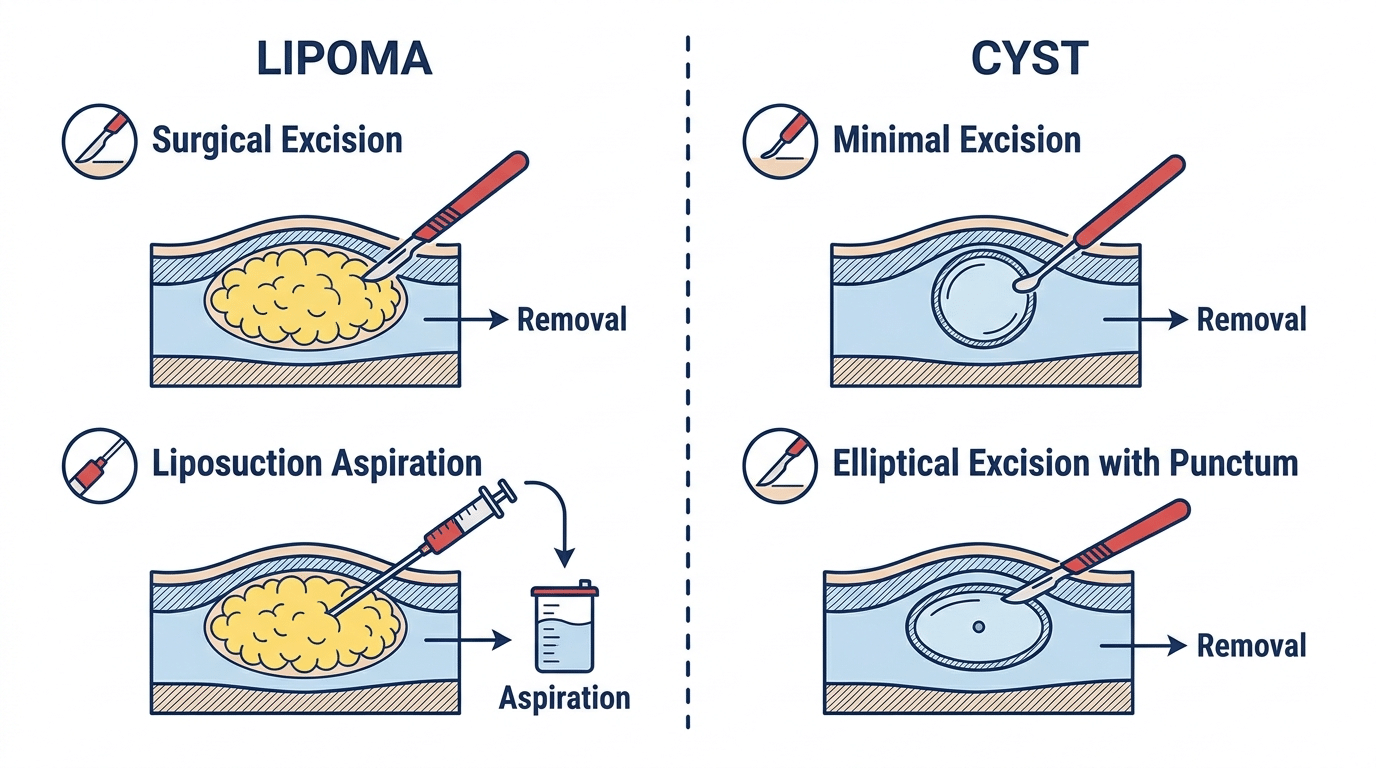
Lipoma removal involves making an incision over the lump, dissecting the lipoma free from the surrounding fatty tissue, and removing it intact within its capsule. The incision length is typically approximately half the diameter of the lipoma. The wound is closed in layers with sutures. In selected cases, liposuction-assisted aspiration can be used through a minimal puncture incision — though this technique carries a higher recurrence rate than formal surgical excision. For more detail, see our post on whether lipoma removal leaves a scar and our post on whether lipomas come back after removal.
Cyst Removal
Cyst removal requires complete excision of the cyst capsule — the fibrous wall that lines the cyst. If any portion of the capsule is left behind, the cyst will reform. For smaller cysts, a minimal excision technique can be used. For larger cysts or those with a history of previous inflammation, an elliptical excision incorporating the punctum is performed. For information on whether a cyst will return, our post on cyst recurrence is worth reading. For guidance on home removal, see our post on whether you can remove a cyst at home.
Frequently Asked Questions
How can I tell if my lump is a lipoma or a cyst?
The key distinguishing features are: feel (lipomas are soft and doughy; cysts are firmer and more spherical); the presence of a punctum (a small dark spot on the surface indicates a cyst, not a lipoma); and behaviour (cysts can become inflamed and painful; lipomas almost never do). A clinical examination by an experienced surgeon is the most reliable way to distinguish the two.
Can a lipoma turn into a cyst or vice versa?
No. Lipomas and cysts are entirely different structures with different cell types and different origins. A lipoma cannot become a cyst, and a cyst cannot become a lipoma.
Do lipomas and cysts need to be removed?
Neither requires removal for medical reasons in most cases. Removal is recommended where the lump is causing symptoms, growing, or causing cosmetic concern. For cysts, elective removal when the cyst is calm is always preferable to waiting for an inflammatory episode to force the issue.
Can a lipoma become cancerous?
No. Lipomas are composed of mature fat cells and do not undergo malignant transformation. Liposarcoma — a malignant tumour of fat cells — is a distinct entity that does not arise from pre-existing lipomas.
Is lipoma removal or cyst removal more painful?
Both procedures are performed under local anaesthetic and are painless during surgery. The injection of local anaesthetic is the most uncomfortable part of both procedures. Post-operatively, both tend to cause mild to moderate tenderness for two to three days, manageable with standard over-the-counter pain relief.
Will my lipoma or cyst come back after removal?
Lipoma recurrence following complete surgical excision is uncommon. Cyst recurrence following complete capsule removal is also uncommon — but if any portion of the cyst capsule is left behind, the cyst will almost certainly reform. Complete capsule excision is the essential technical requirement of cyst removal.
Lipoma and Cyst Removal at Centre for Surgery
Centre for Surgery performs lipoma removal and cyst removal at our CQC-regulated Baker Street clinic in central London. All procedures are performed by GMC-registered consultant plastic surgeons under local anaesthetic as day-case procedures. Every excised specimen is sent for histological analysis as standard. Finance options including 0% APR are available through our partner Chrysalis Finance — visit our Finance Options page for details.
Phone: 0207 993 4849 | Email: contact@centreforsurgery.com | Address: 95-97 Baker Street, London W1U 6RN

[contact-form-7 id=”256″ title=”Treatments form”]