
The words “mole” and “melanoma” are sometimes used interchangeably in everyday conversation, but they describe two fundamentally different things. A mole is a benign collection of pigmented skin cells. A melanoma is a malignant tumour — one of the most serious forms of skin cancer, capable of spreading to other organs if not caught and treated early. Understanding the distinction between the two is not merely academic. It is clinically important, and in some cases it is the difference between a straightforward cosmetic procedure and a life-saving diagnosis.
At Centre for Surgery in London, our surgeons perform mole removal regularly — both for cosmetic reasons and where there is clinical concern about a lesion’s appearance. Every specimen removed at our Baker Street clinic is sent for histological analysis as standard, ensuring that any unexpected finding is identified and acted upon promptly. This guide explains what moles and melanomas are, how they differ, what warning signs to look for, and when to seek a professional assessment.
What Is a Mole?
A mole — medically called a melanocytic naevus — is a benign growth that develops when melanocytes, the pigment-producing cells of the skin, cluster together rather than spreading evenly throughout the epidermis. Moles are extremely common. Most adults in the UK have between 10 and 40 moles on their body, and having moles is entirely normal.
Moles can be present from birth — these are called congenital naevi — or they can develop during childhood and early adulthood. It is normal for new moles to appear up to the age of around 40. After this age, new pigmented lesions should be viewed with slightly more caution and assessed professionally rather than assumed to be benign. Sun exposure accelerates the development of moles and increases the total number a person will develop over their lifetime, which is one of the reasons people with fair skin who have had significant UV exposure tend to have more moles than average.
A typical benign mole has several characteristic features. It is round or oval in shape with a well-defined, regular border. Its colour is uniform — usually a single shade of brown or tan, though some moles are pink, flesh-coloured, or very dark. It is flat or only slightly raised, and its surface is smooth. Most importantly, it is stable — it does not change significantly in size, shape, or colour over time. Benign moles that have been present and unchanged for many years are very unlikely to represent a problem, though any new change in an established mole should prompt a professional review.
Most people who choose to have moles removed do so for cosmetic reasons — the mole is in a visible or irritating location, it catches on clothing or jewellery, or they simply find its appearance bothersome. Cosmetic mole removal at Centre for Surgery is a straightforward, safe procedure when performed by an experienced plastic surgeon using appropriate technique.

What Is a Melanoma?
Melanoma is a malignant skin cancer that originates in the melanocytes — the same pigment-producing cells from which moles develop. It is the most dangerous form of skin cancer because of its tendency to metastasise — to spread via the lymphatic system and bloodstream to other organs, including the lymph nodes, lungs, liver, brain, and bones. When caught at an early stage, melanoma is highly treatable and the prognosis is excellent. Advanced melanoma that has spread to other organs is far more difficult to treat and carries a significantly poorer prognosis.
Melanoma is the fifth most common cancer in the UK, with approximately 16,000 new cases diagnosed each year. It is more common in people with fair skin, a history of sunburn, a large number of moles, a personal or family history of melanoma, or a history of significant UV exposure including sunbed use. However, melanoma can develop in people of any skin type and in areas of the body that are not regularly exposed to the sun, including the soles of the feet, the palms of the hands, and beneath the nails.
Melanoma can develop in two ways: it can arise within a pre-existing mole — causing it to change in appearance — or it can appear as an entirely new lesion on previously normal skin. The latter often presents as a new dark or unusual-looking spot that was not there before. Either presentation warrants prompt professional assessment.
The Key Differences Between a Mole and a Melanoma
Stability vs Change
The single most important distinguishing feature between a benign mole and a melanoma is change. A stable mole that has looked the same for years and continues to look the same is almost always benign. A lesion that has changed — in size, shape, colour, or texture — over weeks or months requires urgent assessment. Change is the hallmark of a malignant process, and it is the feature that most reliably distinguishes a melanoma from a harmless naevus.
Borders
Benign moles have well-defined, regular, smooth borders. The edge of the lesion is clear and consistent all the way round. Melanomas typically have irregular, notched, or poorly defined borders — the edge may appear to blur into the surrounding skin, or it may have a jagged, saw-tooth outline. This irregularity reflects the disordered growth of malignant cells, which do not respect the normal structural boundaries of the skin.
Colour
A benign mole is usually a single, uniform shade of brown, tan, or black. Melanomas characteristically show variation in colour within the same lesion — different shades of brown, black, red, white, or blue may all be present. This colour heterogeneity reflects the irregular distribution of melanin within the tumour and is one of the most recognisable features of a melanoma when examined carefully.
Size
Most benign moles are smaller than 6mm in diameter — roughly the size of the end of a pencil rubber. Melanomas are often larger, and lesions that are growing or that exceed 6mm in diameter warrant assessment. This said, size alone is not a reliable indicator — small melanomas exist, and some large lesions are entirely benign — so size should always be considered alongside other features rather than in isolation.
Symptoms
Benign moles are generally asymptomatic. They do not itch, bleed, crust, or produce discharge spontaneously. As covered in our post on itchy or bleeding moles, occasional irritation from clothing or shaving is not necessarily a sign of malignancy. However, a mole that bleeds without trauma, that itches persistently without an obvious external cause, that develops a crust or scab, or that produces any form of discharge should be assessed promptly.
Surrounding Skin
A benign mole sits cleanly within the surrounding normal skin without affecting it. Melanomas can sometimes produce a halo of redness, inflammation, or satellite lesions — smaller dark spots — in the skin around the main lesion. The development of any visible change in the skin surrounding an established mole is a reason to seek professional review.
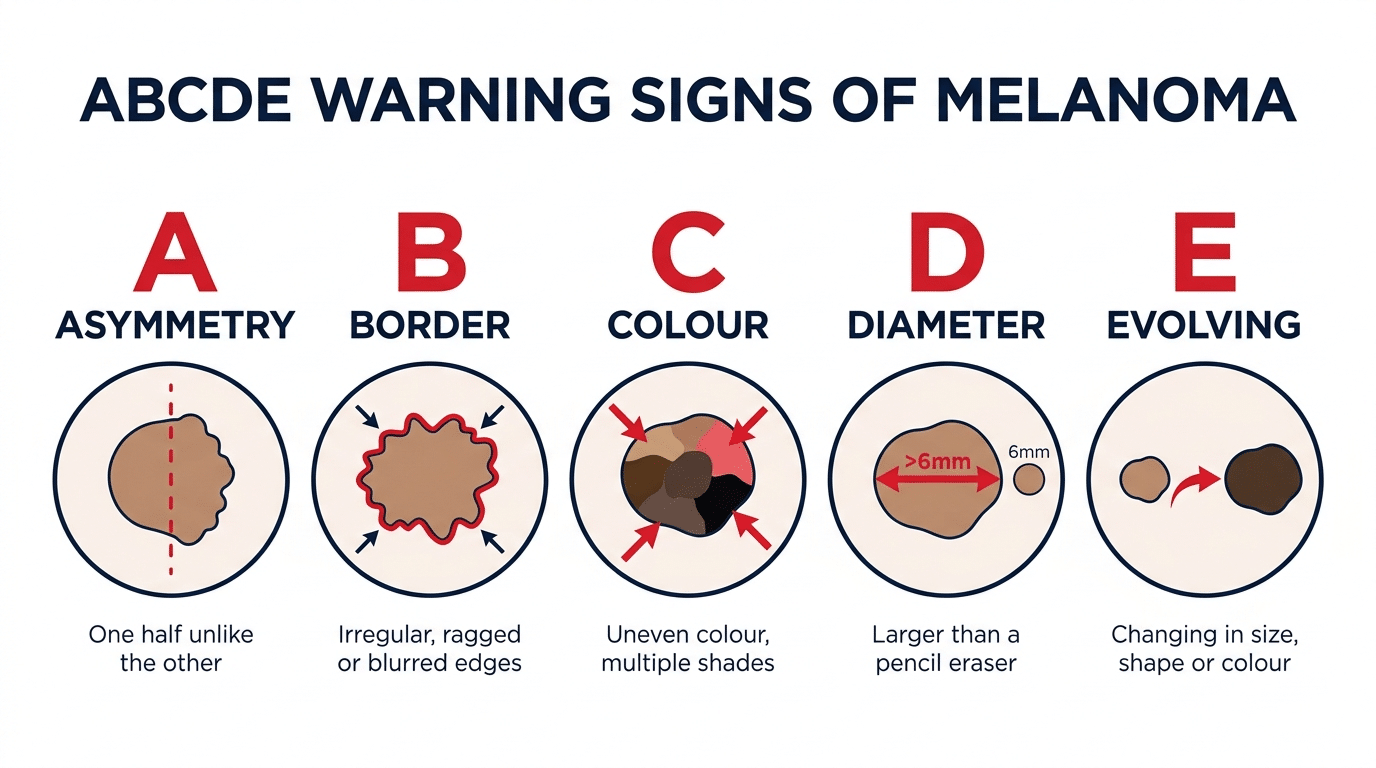
The ABCDE Rule — A Practical Guide
The ABCDE rule is a widely used clinical tool for assessing pigmented skin lesions and identifying features that may suggest malignancy. It is a useful starting point for any self-examination, though it is not a substitute for professional assessment — it is a guide to help identify which lesions need to be seen by a doctor urgently.
A — Asymmetry. If you draw a line through the middle of a benign mole, the two halves should mirror each other. A melanoma is typically asymmetric — one half looks different from the other. Any lesion where the two halves are noticeably different in shape, size, or appearance should be assessed.
B — Border. As discussed above, benign moles have smooth, well-defined borders. Irregular, ragged, notched, or blurred borders are a feature of melanoma.
C — Colour. A single, uniform colour throughout the lesion is reassuring. Multiple colours — varying shades of brown or black, or the presence of red, white, or blue within the lesion — are a warning sign.
D — Diameter. Lesions larger than 6mm merit attention, particularly if they are new or growing. Any lesion that appears to be enlarging should be assessed regardless of its current size.
E — Evolution. Any change in a pre-existing mole — in any of the above features, or in symptoms such as itching or bleeding — is the most important warning sign of all. Melanomas evolve over time; benign moles do not change significantly.
Some clinicians add a sixth criterion: F — Funny-looking. This refers to lesions that simply look different from all the other moles on the body — an outlier that doesn’t fit the pattern of the patient’s other naevi. The “ugly duckling” sign, as it is sometimes called, is a useful prompt to seek assessment even when none of the formal ABCDE criteria are clearly met.
RELATED: Should Every Removed Mole Be Sent for Biopsy?
Other Skin Lesions That Can Be Confused with Moles or Melanoma
The differential diagnosis of pigmented skin lesions extends beyond moles and melanoma. Several other conditions can produce dark or unusual-looking lesions that require professional assessment to distinguish from malignancy.
Seborrhoeic Keratosis
Seborrhoeic keratoses are extremely common benign skin growths that tend to appear in middle age and beyond. They often have a characteristic waxy, stuck-on appearance and can range in colour from pale tan to very dark brown or black. They are frequently mistaken for melanomas by patients because of their dark colour and irregular surface, but they are entirely benign. They can be removed for cosmetic reasons as part of the lumps and bumps removal procedures performed at Centre for Surgery.
Dermatofibroma
Dermatofibromas are firm, benign nodules that most commonly appear on the legs. They are usually light brown to reddish-brown in colour and may have a slightly dimpled surface. While they can look concerning to the untrained eye, they are benign and usually require no treatment unless they are causing symptoms or cosmetic concern.
Basal Cell Carcinoma
Basal cell carcinoma (BCC) is the most common form of skin cancer in the UK, though it is far less dangerous than melanoma as it very rarely metastasises. BCCs often appear as a pearly, translucent, or skin-coloured nodule, sometimes with small blood vessels visible on the surface, or as a flat, scar-like lesion. Occasionally they have pigmented variants that can be confused with melanoma. Any unusual lesion — particularly one that is growing, ulcerating, or not healing — should be assessed professionally.
Blue Naevus
Blue naevi are benign pigmented moles with a characteristic blue-grey colour caused by the deep location of melanocytes within the dermis. Their unusual colour can cause concern but they are benign in the vast majority of cases. Atypical or rapidly enlarging blue naevi should be assessed.
When Should I Have a Mole Assessed?
You should seek a professional assessment of any pigmented skin lesion if you notice any of the ABCDE features described above — particularly asymmetry, irregular borders, colour variation, a diameter greater than 6mm, or any evolution in an established lesion. You should also seek assessment for any new lesion that appears after the age of 40, any mole that bleeds without obvious external cause, any lesion that is growing or that simply looks different from all your other moles, and any pigmented area that does not heal after several weeks.
When you present for assessment at Centre for Surgery, your lesion will be examined carefully by an experienced plastic surgeon. Dermoscopy — a non-invasive technique using a handheld illuminated magnifier — allows close examination of the internal structure of a lesion in a way that is not possible with the naked eye. Where there is any clinical concern, excision with histological analysis is the gold standard for definitive diagnosis. Our surgeons take a conservative approach: when in doubt, they excise. The consequences of a missed melanoma vastly outweigh the minor inconvenience of removing a lesion that turns out to be entirely benign.
RELATED: Why Choose a Plastic Surgeon for Mole Removal?
How Is a Suspicious Mole Removed and Assessed?
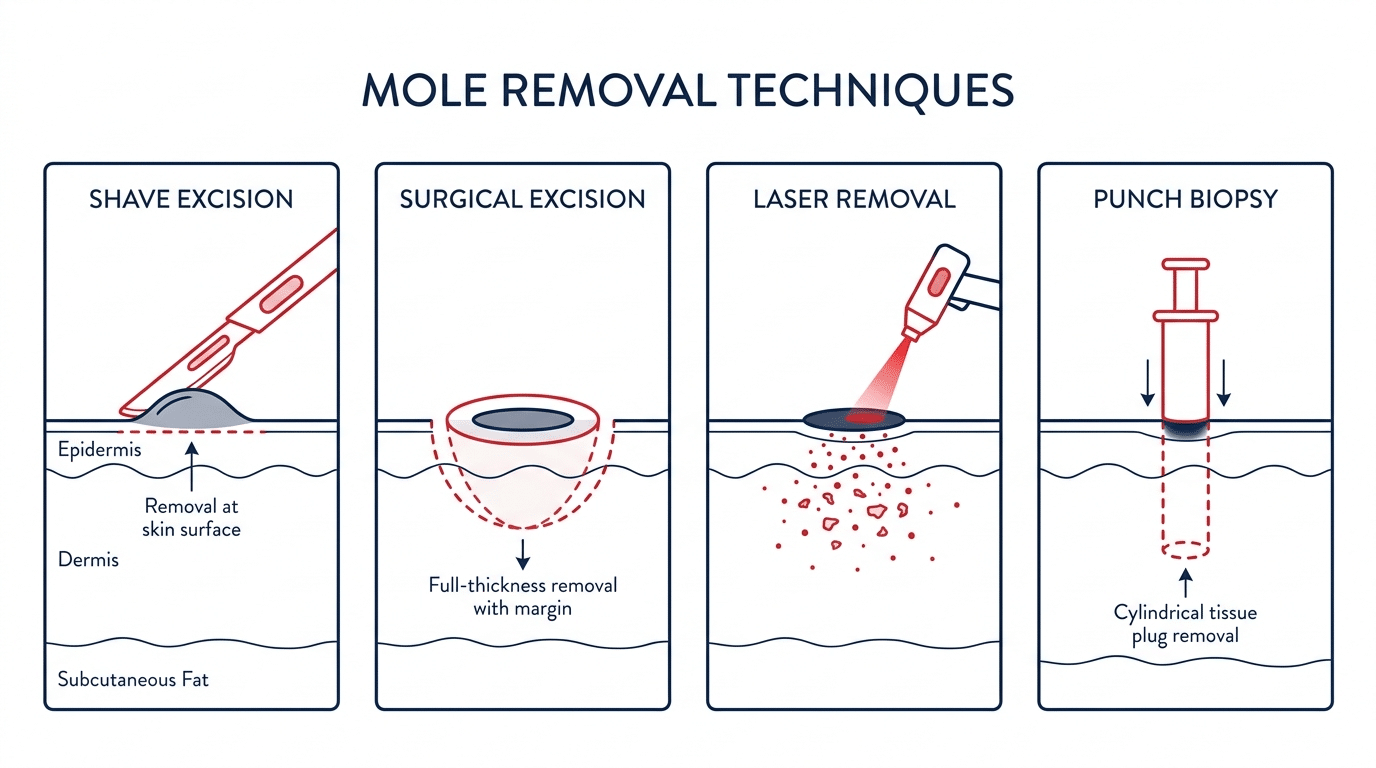
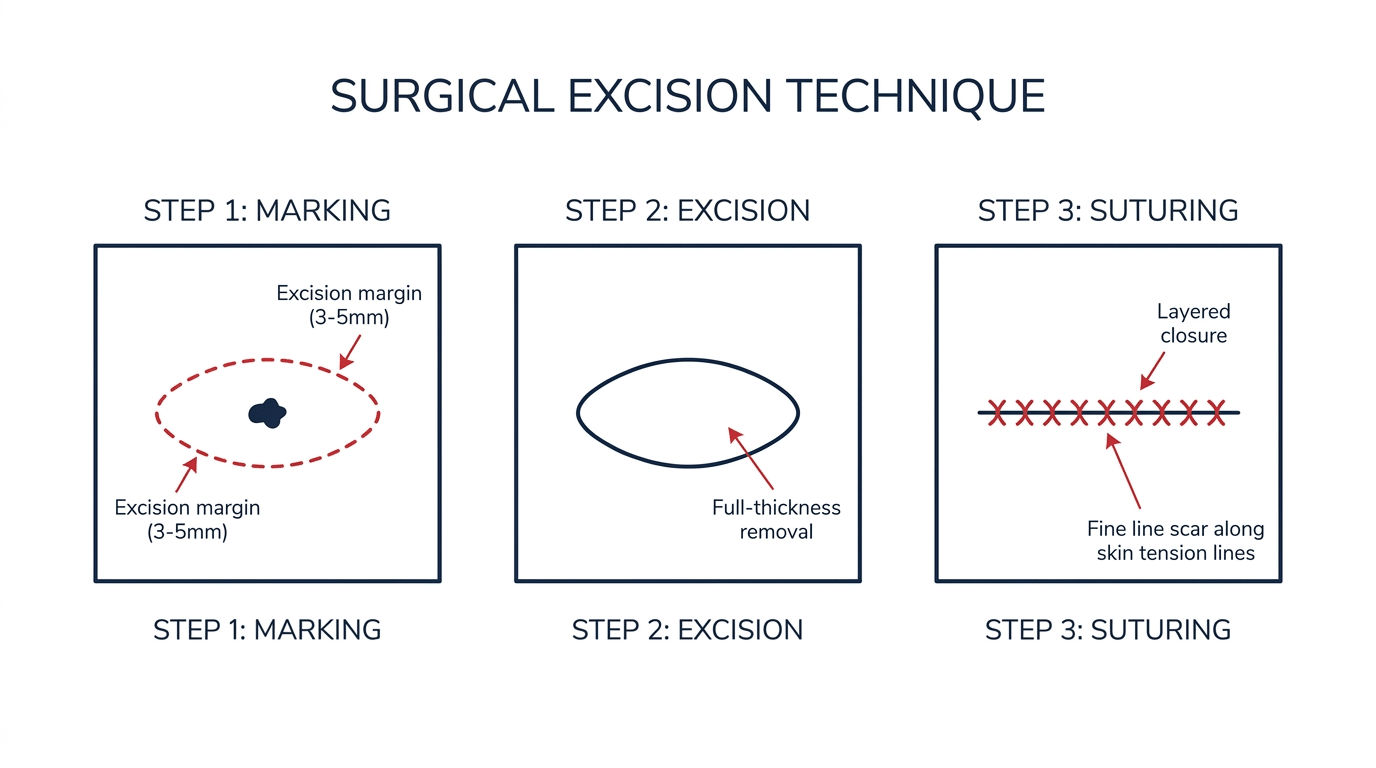
When a mole is assessed and the clinical decision is made to remove it, the procedure is performed under local anaesthetic as a day case at our Baker Street clinic. For a lesion that is clinically suspicious, excision with a margin of surrounding normal skin is performed — this ensures that any abnormal cells at the periphery of the lesion are captured within the excised specimen. The specimen is then sent to a pathology laboratory for histological analysis by a consultant histopathologist.
Histological analysis provides a definitive diagnosis — it identifies the exact nature of the lesion at a cellular level and, in the case of a melanoma, determines the depth of invasion (Breslow thickness) and other prognostic features that guide subsequent management. If a melanoma is confirmed, the results are discussed with the patient and an appropriate treatment plan is put in place, which may involve wider local excision and referral to a specialist skin cancer multidisciplinary team.
At Centre for Surgery, all excised tissue — not just suspicious lesions — is routinely sent for histological analysis. This standard of care means that patients receive a confirmed diagnosis for every lesion removed, providing both clinical reassurance and the safety net of pathological oversight.
RELATED: Can All Moles Be Safely Removed?
Can Mole Removal Cause Melanoma to Spread?
This is a concern patients sometimes raise, and it deserves a direct answer. There is no reliable clinical evidence that performing an excision biopsy of a melanoma causes it to spread. The theoretical concern — that cutting into a malignant lesion could seed cancer cells into the bloodstream or lymphatics — has been studied extensively, and the current consensus is that excision biopsy does not worsen outcomes. What is critically important is that excision is complete and that the specimen is sent for histological analysis so that the diagnosis can be established and treatment planned appropriately. Delaying removal out of concern about spreading is not clinically justified. For more on this topic, see our guide to why every removed mole should be sent for biopsy.
Mole Removal on the NHS vs Private Treatment
As discussed in our guide to mole removal on the NHS, the NHS will generally only remove moles that are clinically suspicious for malignancy or that are causing a documented functional problem. Cosmetic mole removal — where the lesion appears benign but the patient wishes to have it removed for aesthetic reasons or peace of mind — is not routinely funded by the NHS. Patients who have a lesion they wish to have assessed or removed will need to do so privately.
Private mole removal at Centre for Surgery is accessible, straightforward, and includes histological analysis as standard. Finance options including 0% APR through Chrysalis Finance are available — visit our Finance Options page for details.
Frequently Asked Questions
How do I tell if a mole is cancerous at home?
Use the ABCDE rule as a guide: look for Asymmetry, irregular Border, Colour variation, Diameter greater than 6mm, and Evolution (change over time). Any lesion that meets one or more of these criteria, or that simply looks different from your other moles, should be assessed professionally. Self-examination is a useful tool for identifying lesions that need attention, but it is not a substitute for professional assessment and dermoscopy.
Can a normal-looking mole be melanoma?
Yes, in a small number of cases. Some melanomas — particularly nodular melanomas — can grow quickly and may not show all the typical ABCDE features, particularly in their early stages. This is why any new or changing lesion should be assessed professionally even if it does not look obviously abnormal.
What does a melanoma feel like?
In early stages, melanoma often produces no symptoms at all and cannot be distinguished from a benign mole by feel alone. More advanced lesions may feel firm, raised, or nodular. Some melanomas itch, bleed, or develop a surface crust. The absence of symptoms does not mean a lesion is safe — visual assessment and dermoscopy are the primary diagnostic tools.
How quickly does melanoma develop?
This varies considerably between subtypes. Superficial spreading melanoma — the most common type — typically grows slowly over months to years before becoming invasive. Nodular melanoma is more aggressive and can progress rapidly over weeks to months. Any new or changing pigmented lesion should be assessed promptly rather than watched and waited — early treatment is always more effective.
Can melanoma look like a normal mole?
Yes. In its earliest stages, a melanoma arising within a pre-existing mole may look very similar to the mole itself, with only subtle changes distinguishable by dermoscopy. This is one of the reasons why regular self-examination and professional review of any changing lesion is important.
Does having lots of moles increase my melanoma risk?
Yes. Having more than 50 moles is an established risk factor for melanoma, as is having a large number of atypical moles. This does not mean that melanoma is inevitable, but it does mean that regular self-examination and periodic professional review is advisable.
Mole Assessment and Removal at Centre for Surgery
Dr Spyridon Vlachos is a Consultant Plastic and Reconstructive Surgeon at Centre for Surgery with extensive experience in the assessment and surgical management of pigmented skin lesions. With over 25 years of specialist experience, Dr Vlachos brings exceptional precision and clinical judgement to every procedure. He is a recognised specialist on the GMC’s plastic surgery register and a member of the International Society of Aesthetic Plastic Surgeons.
All mole removal procedures at Centre for Surgery are performed at our CQC-regulated Baker Street clinic in central London. Every excised specimen is sent for histological analysis as standard. If you are concerned about a mole or pigmented skin lesion, or wish to have a mole removed, contact us today to arrange a consultation.
Phone: 0207 993 4849 | Email: contact@centreforsurgery.com | Address: 95-97 Baker Street, London W1U 6RN
Finance options including 0% APR are available through our partner Chrysalis Finance — visit our Finance Options page for details.

[contact-form-7 id=”256″ title=”Treatments form”]



