Saddle nose deformity is a condition in which the bridge of the nose appears sunken or concave, resembling the shape of a saddle. The dip in the nasal structure can affect both the appearance of the face and the function of the nose — breathing difficulties are common when the nasal valves are compromised. Specialist rhinoplasty is the standard treatment for both the aesthetic and the functional consequences.
RELATED: Cosmetic vs Functional Rhinoplasty
This article covers what saddle nose deformity is, what causes it, the symptoms it produces, and the surgical options for correction.
What Is a Saddle Nose Deformity?
Saddle nose deformity is a loss of structural support in the nasal framework that causes the bridge to collapse inward. The collapse can range from a subtle indentation to a pronounced concavity affecting both appearance and breathing.
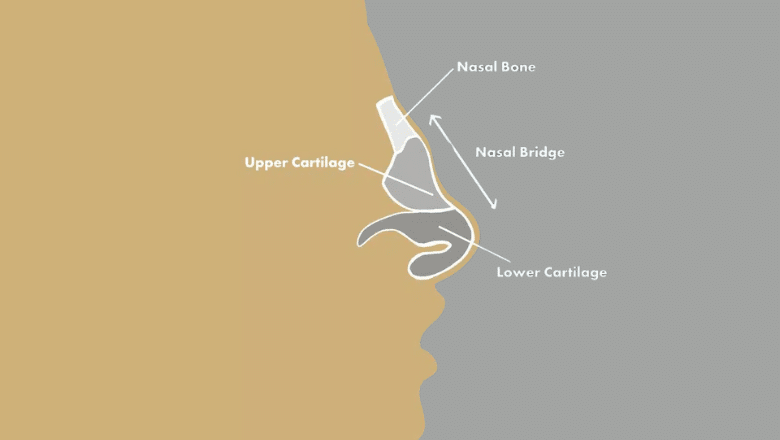
The structures that maintain the shape of the nose — the nasal septum, the upper lateral cartilages, and surrounding soft tissue — work together to support the nasal bridge and keep the airway open. Damage to any of these can produce a saddle nose. Severity depends on how much support has been lost and whether one or several supporting structures are involved.
RELATED: Different Types of Nose Shapes
What Causes Saddle Nose?
There are four main causes, in roughly descending order of frequency.
Trauma
Direct trauma to the nose — sports injuries, falls, road traffic accidents, or assault — is the most common cause. Nasal fractures, septal cartilage damage, and untreated septal haematomas can all lead to progressive collapse of the bridge over weeks or months. A septal haematoma in particular can destroy septal cartilage if not drained promptly, which is why any blunt nasal trauma should be assessed early.
Post-Rhinoplasty Complications
Saddle nose deformity can occur after rhinoplasty, particularly when too much cartilage or bone has been removed without adequate structural reinforcement. The collapse may be immediate or develop gradually over months or years. Revision rhinoplasty with cartilage grafting is the usual treatment.
RELATED: What Is Considered a Bad Nose Job?
Inflammatory and Autoimmune Disease
Several inflammatory and autoimmune conditions can erode nasal cartilage and produce saddle nose deformity. The most common are granulomatosis with polyangiitis (formerly Wegener’s), relapsing polychondritis, and systemic lupus erythematosus. Cocaine use can also cause progressive cartilage destruction through repeated inflammation and ischaemia.
When an inflammatory or autoimmune cause is suspected, surgical correction is usually deferred until the underlying disease is stable, since active disease can destroy the cartilage grafts placed during reconstruction.
Congenital
Less commonly, saddle nose deformity is congenital. It can occur as part of certain genetic syndromes (including congenital syphilis, where it has historically been a recognised feature) or as an isolated developmental anomaly affecting the nasal cartilage.
Symptoms of Saddle Nose Deformity
The symptoms fall into two groups: structural appearance and nasal function.
The structural changes are usually visible — a depression along the nasal bridge, sometimes extending toward the tip, with possible asymmetry of the nostrils in more severe cases. The supratip area may appear pinched or over-rotated.
The functional symptoms are caused by collapse of the internal nasal valves, which control airflow into the nose. Patients commonly report nasal obstruction, difficulty breathing through the nose during exercise or sleep, mouth-breathing at night, snoring, and chronic congestion. These symptoms tend to worsen as the structural collapse progresses.
Surgical Correction
Rhinoplasty for saddle nose deformity rebuilds the nasal bridge using cartilage grafts, restoring both the contour and the structural support to the internal nasal valves. The operation is performed under general anaesthesia and typically takes three to four hours, depending on the severity of the deformity. Most patients are discharged the same day.
The surgical approach varies with the severity of the deformity.
Mild Saddle Nose
Subtle depressions can often be corrected with reshaping of the existing upper lateral cartilages and a small fascia or cartilage onlay graft to smooth the contour of the bridge. Recovery is straightforward and the result is usually predictable.
Moderate Saddle Nose
Moderate cases require dedicated cartilage grafts. Spreader grafts are placed between the septum and upper lateral cartilages to widen the internal valve, and dorsal onlay grafts rebuild the bridge contour. Septal cartilage is the first choice when available; ear (conchal) cartilage is the second.
Severe Saddle Nose
Severe collapse requires more substantial reconstruction, usually with rib (costal) cartilage. Rib cartilage provides the volume and strength needed to rebuild a significantly collapsed bridge, and is reliable in the long term. Diced cartilage wrapped in fascia is a common technique for the dorsal onlay in these cases, producing a smooth contour without visible graft edges.
Cartilage Grafts vs Synthetic Implants
Surgeons at Centre for Surgery use the patient’s own cartilage rather than synthetic implants for saddle nose reconstruction. Autologous cartilage integrates with surrounding tissue, has a very low long-term complication rate, and avoids the infection and extrusion risks associated with synthetic implants such as silicone or Gore-Tex.
RELATED: What Is Augmentation Rhinoplasty?
Recovery After Saddle Nose Rhinoplasty

Recovery from rhinoplasty for saddle nose deformity follows the typical pattern for major rhinoplasty, with some additional considerations because of the cartilage grafting involved.
The first one to two weeks involve nasal swelling, bruising around the eyes, and a degree of nasal congestion. A nasal cast or splint is worn for the first week. Most patients return to desk-based work after 10 to 14 days.
By six weeks, the majority of visible swelling has settled and breathing has usually improved noticeably. The internal nasal valves are now better supported and patients often report the most significant functional benefit at this stage.
Final results take 9 to 12 months to fully appear, particularly at the tip. The cartilage grafts settle and integrate with surrounding tissue over this period, and the contour of the bridge becomes progressively more refined.
If rib cartilage was used, the chest donor site usually causes mild discomfort for the first one to two weeks and leaves a small scar (typically 3-4cm) along the natural skin crease.
FAQs
Is saddle nose deformity serious?
It isn’t life-threatening, but progression depends on the cause. Saddle nose due to active inflammatory disease can worsen over time if the underlying condition isn’t controlled. Saddle nose from healed trauma or completed rhinoplasty is usually stable. Functional symptoms (nasal obstruction, mouth-breathing, snoring) tend to be the more troubling consequences for most patients.
Can rhinoplasty for saddle nose be combined with a facelift?
Yes. Rhinoplasty and facelift can be performed in the same operation in suitable patients, which avoids two separate recovery periods. Suitability depends on overall health, the complexity of each procedure, and the surgeon’s assessment.
Will rhinoplasty improve breathing if I have a saddle nose?
In most cases, yes. Reconstructing the nasal bridge restores support to the internal nasal valves, which is where most of the airway resistance in saddle nose deformity comes from. Patients with significant pre-operative obstruction usually report substantial functional improvement after surgery.
Can saddle nose deformity heal on its own?
No. Once structural support is lost, the deformity is permanent without surgical correction. Inflammatory causes may stabilise with medical treatment but the existing collapse won’t reverse on its own.
Are there any non-surgical alternatives?
For patients not suitable for surgery, dermal filler can be used to improve the contour of the bridge cosmetically. This is a temporary measure that doesn’t address the structural cause or improve breathing — it’s a camouflage option, not a treatment.
Centre for Surgery
Centre for Surgery is a CQC-regulated cosmetic surgery clinic at 95–97 Baker Street, London W1U 6RN. Saddle nose rhinoplasty is performed by GMC specialist-registered consultant plastic surgeons with specific experience in complex and revision nasal surgery, using autologous cartilage grafts.
Finance is available through Chrysalis Finance, with 0% APR options.
To arrange a consultation, call 0207 993 4849 or email contact@centreforsurgery.com.

[contact-form-7 id=”256″ title=”Treatments form”]